Athletic Training, Baseball, Basketball, Football - American, Health, Physical Therapy, Pickleball, Rehab, Tennis, Volleyball
How to Identify and Treat Sprained Ankles


Dr. Sophia Deben is a board-certified orthopedic surgeon and foot and ankle specialist.
“Today, we're going to talk about ankle sprains.
This is the first part of a multi-part series. So stay tuned for parts two, three, and maybe four. Let's talk today about what is an ankle sprain.
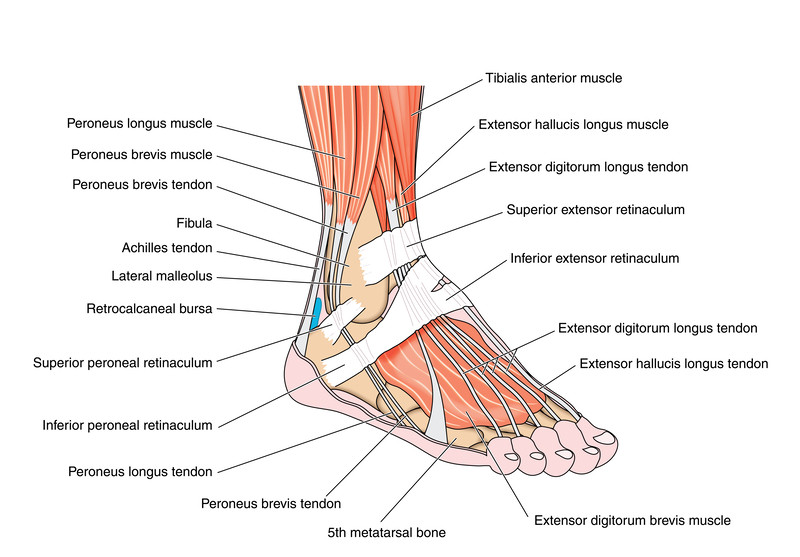
An ankle sprain essentially is when the foot goes out of the plane of the leg. The leg bone or the tibia is in front and goes up and down. The skinny bone on the outside of the ankle is the fibula. And then the round bone in the center is the talus.

Bones are individual structures. They're connected by thick cords called ligaments. The three main ligaments that we injure with an ankle sprain are the deltoid on the medial or inside of the anterior tail of the fibular ligament on the outside, and the calcaneus fibular ligament, about 80% to 90% of ankle sprains are inversion, where the foot goes inwards towards the medial side of the ankle.

But sometimes, we do have inversion sprains. A sprain is an injury to a ligament. We qualify them as mild, moderate, or severe, sometimes also known as a grade one, Grade two, or grade three sprain. A grade one sprain is a gentle stretch. A grade two sprain is a partial tear, and a grade three sprain is a complete tear.
The diagnosis of the severity of the sprain in relation to what tissue is torn doesn't come until much later. Most of the time, when someone sprains an ankle, there's so much pain swelling, and inability to move the ankle that assessing the ligaments either clinically by pulling on them or getting into an MRI scanner is not quite feasible or appropriate.
70 to 80% of all ankle sprains resolve by themselves, usually with some physical therapy.
Only about 20% of ankle sprains require any kind of surgical management, and those are patients who ignore their first ankle sprain and probably their second. And they come and see me after the third or fourth.
So, the critical key point here about ankle sprains is not to avoid them. You're going to play your sport. The turf is going to be wet, and somebody's foot is going to be underneath you. That happens.
However, you need to get appropriate treatment after your first one so you don't have a second, third, or fourth. The reason that we keep spraining our ankles after our first sprain is not because of the ligament injury. It's because of another event that happens in our body.
It's a protective reflex. It's called reflex inhibition.
Essentially, if we hurt a body, part, could be our hand, could be our elbow, could be our foot.
The body neurologically or in the nerves turns off the nerves to the muscles of that body part. So if you've injured something in the past, you may notice that you have trouble moving it. That's not because you're being weak or because of pain, it's because the body has reflexively stopped the motion by turning the nerves off to those muscles.
That reflex inhibition is very powerful, specifically with ankle sprains and in the foot. On the outside of the ankle are the two peroneal muscles, the brevis and the longest muscles become dynamic stabilizers.

What that means is that when we're walking, playing sports, or changing direction, we're not relying on the ligaments. We're relying on the muscles. So, if the muscles are turned off or half asleep because of the ankle sprain event that we had three days ago, guess what's going to happen next time you try to stress your ankle? It's going to give, and you're going to have to bypass your dynamic stabilizer because it's not working.
And so one of the critical points to ankle sprains is to reestablish normal firing of the perennial tendons. We need to turn the peroneal tendons back on, and usually, that requires a little bit of physical therapy.
So, as we go through this series, you'll hear me talk about physical therapy for the ankle regularly because it is the number one treatment and the number one preventative to future ankle sprains and, ultimately, future surgery.
What do we do if you're a player and you twisted your ankle? Whether it hurts a little bit or hurts a lot, probably a good idea to tell your coach or your parent, let them evaluate you, and determine whether you can keep playing, keep working out or stay in the game.
If you're a coach and or supervising the player's student during this time period, it's probably a good idea to let them sit down and rest for about 2 to 5 minutes, to evaluate the ankle. At that point, is it swollen like a balloon or is it not really swollen? Is there a lot of bruising or no bruising?
If you feel that there isn't a lot of bruising and swelling, you can evaluate the ankle very simply with three simple tests. One is ankle motion, which is essentially having the patient move it up and down. With the ankles, move both sides equally up, equally down, and smoothly. If one side moves smoothly and the other side doesn’t, that player can't go back into play--the nerves are off, and we need to turn them back on with therapy.

The next is circles to the right and circles to the left once again for smoothness and completeness.
Finally, a single-leg stand and hop would be your third and final functional test to determine if they can go back to play. So if they twisted the left ankle, have them stand on the left leg unsupported and see if they can tolerate that.
If they don't have pain and they feel comfortable in that position, have them take two or three hops on that left side and see if they can tolerate it. If they have no pain and they feel solid on the ankle, I think it's perfectly fine for them to go back to play.
If, however, they can't complete any of those three tests or the ankle is very swollen and bruised, we want to institute what's called the RICE protocol.
Rest, ice compression, and elevation.

So rest means not playing. Ice means trying to pack that ankle down with ice front, side, and back as much as you can for about 20 minutes. Compression means trying to apply a little bit of tightness around the ankle, perhaps with an E strap or an elastic bandage, and elevation, making sure the foot is higher than the heart, which allows all of the swelling to drain downhill.


FlexiKold Gel Ice Pack
If the player can't bear weight, crutches would be reasonable. So, mom and dad, when you receive your player after practice or a game and the ankle is big and swollen and purple, they are uncomfortable, and they're on crutches, probably the first thing to do is to tuck them in bed and or the couch with their foot higher than their heart and a cooler full of ice next to them, replacing the ice 20 minutes on, 20 minutes off.
At that point. I would also recommend if they're medically able to take an ibuprofen, whatever dose is appropriate for their age and weight. You also probably want to repeat that dose before bedtime. Examine your player the next morning. If they're still really swollen or bruised, I'd probably recommend medical attention. Also, if they're limping or they're not walking, normally I'd recommend evaluation by a medical provider.
About 20% or one in five ankle sprains is an ankle fracture. And we don't want to be walking around on a broken ankle. So those are your first 24 hours, some typical key findings, and then what to expect later, maybe physical therapy and proprioceptive retraining, or balance retraining to get back in the sport
Thanks. We'll be back with part two.”




