Health
Welcome and thanks for visiting...

Shoulder Injuries in Sports Part II

In the last article, we started discussing another common area of injury in sports, especially the overhead athlete (volleyball, tennis, baseball pitcher, etc), the shoulder. In starting our discussion, we talked about the anatomy of the shoulder that is commonly involved or impacted in sports. This is important to know because the time that it takes you to recover can depend on the injury that occurs and what structures are involved. Keep in mind, the information in this blog should never replace the advice of your medical provider. Nothing can replace a physical examination with your health care provider.
In this week's discussion, we will start to look at how those structures are involved and what positions usually injure these areas. Keeping in mind there are a lot of movements that can injure the shoulder and this will not be an all-inclusive list. What we will do is go over the most common ones we see in the clinic and the tissues that are involved.
Pop in the shoulder – sometimes an athlete will do an activity which causes a pop in the shoulder. This can happen with a variety of sports and activities. For the volleyball player this may happen when they are performing an overhead serve and feel a pop in the shoulder. For the baseball player, this may happen when they throw a hard pitch and feel a pop in the shoulder. For the football player, this maybe when they collide with another player and feel a pop in the shoulder. A pop in the shoulder does not always mean the same thing. Lot depends on the position the arm is in, what the mechanism is that caused the pop (throwing versus being hit) and if there are any other symptoms associated with the pop.
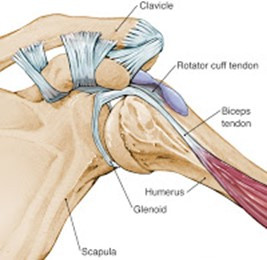
When looking at the shoulder, there are several specific structures that can be involved. This can include but is not limited to the clavicle, biceps tendon, rotator cuff and labrum of the shoulder.
In the absence of a fracture, some of the most common presentations we see are:
- Pop in the shoulder and balling up of the muscle on the front of the arm - typically this is associated with a biceps rupture. This is a hard one to miss as there is typically a lot of pain, more diffuse pain, bruising in the arm (usually in the next 48-72 hours) and balling up of the bicep muscle (Popeye bicep). The balling up of the muscle is a dead giveaway of what is going on. In this case you should see your physician, and this will likely require a surgical intervention.
- Pop in the shoulder with pain on top of shoulder with deformity – this can be associated with an AC (acromioclavicular) joint dislocation. We will discuss this more next week but this will result in point tenderness on the top of the shoulder with a visible difference when comparing to your opposite shoulder.
- Pop in the shoulder with pain in front of shoulder - this can be associated with a lesser of a degree of bicep tear or labral tear. This will result in more localized pain, to the front of the shoulder. If bruising occurs, more likely bicep. If shoulder feels unstable (feels like comes in and out), this can be a sign of larger labral tear. If this is the case, you should see your MD. If no bruising in 24-48 hours, pain resides, there is no loss of shoulder motion and shoulder feels stable, this can most likely be self-treated with ice and shoulder exercises.
- Pop in shoulder without pain - there are a lot reasons you can get a pop in the shoulder. However, if there is no pain, you have full range of motion and no change in strength, you should be good doing activities that do not bother you. I would suggest take it easy and ice proactively.
- Shoulder pops out - this is shoulder dislocation. If itself reduces (goes back in) you should have it checked out by your physician. If it does not self-reduce (stays out of place) this is considered a medical emergency and should be seen right away. There is the possibility of compromised blood flow and neural input to the lower arm and should be relocated (put back in place) ASAP.
- Pop in shoulder with tingling and numbness down the arm – in the shoulder, there is a plexus of nerves that sits in front of the shoulder called the brachial plexus. Sometimes if the upper arm is stretched out to far quickly (trying to grab onto player as they run by) or the shoulder dislocates, this can stretch or compress this nerve complex. This can cause dead arm (feeling like you can’t lift it), tingling and numbness down the arm or loss of strength of the arm. This should be evaluated by your physician ASAP.
*If you have constant and significant tingling and numbness down your arm, loss of sensation in your arm, loss of strength or function of the arm, loss of circulation in your arm (fingers or limb becomes cold to the touch), seeking a medical evaluation is strongly encouraged.*
With sports related shoulder injuries shoulder, the most common tissues involved are the rotator cuff, labrum and long head of biceps. These are often the result of poor training technique, overuse or direct trauma
- Rotator cuff injuries. >80% of rotator cuff injuries occur in the supraspinatus. This will result in pin point pain on the outside of the shoulder (lateral aspect in the subacromial space) and may refer to your deltoid insertion (down the outside of your arm). This will be painful to resistance to the external rotation (rotating the arm out) or raising your arm out to the side. A physician visit is advised if you hear a pop in the shoulder with any of the following: significant pain in the shoulder (5/10 pain or greater), loss of range of motion of the shoulder (unable to move it overhead), significant pain (5/10 or greater) with moving your arm, tingling and numbness down the arm or inability to sleep or lay on that arm at night.
- Long head of biceps tendon. Due to the attachment and crossing of the shoulder joint and how the bicep functions during activities, this is often involved. A physician visit is advised if you have any of the following: pop in shoulder with bruising down the arm or balling up of the biceps, inability to flex the arm, significant pain (5/10 pain or greater) in the arm or with trying to raise the arm or significant pain (5/10 pain or greater) with turning door handles, screwdriver or getting gallon of milk out of the fridge (all very active biceps activities).
- Labral injuries. This is a common injury in sports. Most think if their labrum is torn that this will require surgery. I can tell you that I have treated a lot of athletes (high level and not so high level) and this is really dependent on the location and severity of the tear. Personally, I tore mine in my 30s. As a weightlifter and someone that does Muay Thai and Jiu Jitsu and is over 50, I have not had my repaired. If you have pain that limits your range of motion, prevents you from sleeping at night or your shoulder feels unstable (sensation comes in and out), then you should see a physician.
As with any injury, you can monitor your progress by how your pain is progressing or regressing. You should also start icing right away, 15 min 3+ times per day and cold enough to make you numb in 5 min. The more you ice and the more likely you are to return to your sport and full training quicker and with less problems.
We hope you continue to enjoy this series and find the information valuable. Next week, we will talk a few more injuries then move into some specific stretches and exercises for preventing injuries. If you did enjoy, please share with your colleagues, coaches and training partners and please be sure to follow me on instagrm @ bjjpt_acl_guy and twitter @acl_prevention. #ViPerformAMI #ACLPlayItSafe
Read more:




