Health
Welcome and thanks for visiting...

Shoulder Injuries Part III

In the previous article, we discussed some specific shoulder injuries that can occur and some of the common structures involved with particular injuries. Unfortunately, many of these sporting activities puts the shoulder in its end range of motion and the supporting tissues (rotator cuff, biceps, etc.) in their elongate positions. Therefore, when you try to contract and provide maximal force, the muscle is in an elongated weakened position and more susceptible to injury. In the next article, we will talk about some specific strategies to help increase shoulder range of motion (which helps in reducing risk for injury) and strengthening of the shoulder muscles, so they are less susceptible to injury.
In this article, we want to look at two more injuries, one in the shoulder and one that is often misdiagnosed. In the shoulder is a joint called your AC joint or acromioclavicular joint. We talked about this briefly in our first part of this series, but this is a common enough of an injury that it is worth discussing here in some more detail.
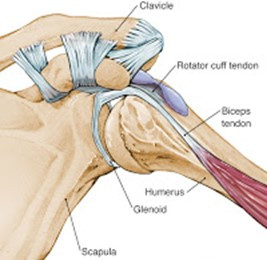
The AC joint is held together by a ligament (depicted in this picture). An AC joint injury is an injury to this ligament where the ligament is torn and allows the clavicle to migrate upwards. One of the most common mechanism of injury of this ligament is a fall on the shoulder or onto an outstretched hand. Most commonly occurs with diving for a ball or having an opponent land on you.
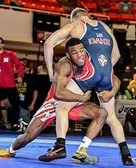
In the case of falling on your shoulder, like in wrestling, this can happen on the person shooting for the takedown or the opponent. For those shooting for the takedown, if they are shooting for a double leg takedown (as depicted here) and their head is in the proper position (head up on the outside) when they drive backwards or at a diagonal, it is not uncommon to land on the shoulder. If this impact is more toward the top of the shoulder, the driving force is directly through the acromion and the clavicle. This puts a lot of stress on the ligamentous structures of the AC joint and can cause an AC separation. AC separations can occur in varying degrees. For a classifications of AC separations, please refer to our previous blog in this series. The other common mechanism of injury for the AC joint is the opponent that is being taken down. Sometimes out of instinct, the opponent being taken down will reach out his arm to break the fall and end up landing on the shoulder.
In either situation, the athlete will commonly feel a sharp pain that will be localized to the small area on the shoulder. If there is separation and depending on the grade, the athlete may see a deformity of the area. The picture below shows two ends of the spectrum. From a low grade level I separation to a grade III - IV. I have included this picture so you can see what this looks like and be able to recognize this when or if you see it in the mirror. Looking in the mirror, you compare your non-involved shoulder to the involved or painful shoulder. You are look at the top of the shoulder where the arrow indicates. Sometimes, it is helpful to have someone else look at as well if you are unsure. 
In the first instance, although painful, this can most likely be treated conservatively. In the second case, this individual should see a health care provider. In either instance, use of an ice massage is very effective at reducing inflammation and pain. For this you can purchase a cyrocup (depicted here) on Amazon or eBay for ~$10. I prefer these over the metal round balls being sold in some circles and here is why. What makes this form of icing so effective is when the ice melts it forms a layer of water between the skin and the ice cube. This layer of water conducts the cold much more efficiently than just ice on the skin or cold metal. This means deeper more effective penetration and colder temperatures are achieved. This results in better inflammation control.

Another injury (not in the shoulder but worth mentioning here) is a rib subluxation. Rib subluxations primarily occur at the costovertebral joint. This will often occur in an overhead athlete (baseball pitcher) or combat athlete when throwing a punch. This can result when your arm is thrown straight out in front of you with a combination of truck rotation. It can also happen if you are pulling your arm back against a lot of resistance rapidly. An example of that is the wrestler who reaches around your opponent (getting an underhook during wrestling) and they resist you or posture up a lot of force. Commonly it is this outstretched position with thoracic rotation followed by maximal muscle contraction that will cause this joint sublux. Where you will feel this is in a pinpoint location in the back or upper back which may radiate up or down the back or around the ribs. One of the key indications is you will get a sharp (sometimes debilitating) pain with a deep breath, cough or sneeze. Inflammation reduction (ice) is important to allow the tissues to relax and allow the joint to self-reduce (which sometimes it does). Use of an ace bandage around the ribs will often help to compress the joint and provide some stability while it is inflamed. If it does not self-reduce, you can see a chiropractor or PT to help put the joint back in position. The same strengthening exercises we recommend with the shoulder will help with this as well.
One common injury in wrestlers and Jiu jitsu is athletes is an oblique or intercostal strain. This happens a lot when you have your opponent in your guard, and you reach for cross collar or across your midline to pull them down or when doing a bump sweep. This injury will often occur where the oblique muscle attaches to the rib cage and will be tender to the touch at the intersection of the ribs and abdominal muscle. This injury will hurt a lot when you sit up and when you take a deep breath or sneeze. Due to the location of the pain and the orientation of the symptoms, this is often misdiagnosed as a rib injury. Two very different injuries and two different treatment approaches. It is for that purpose that I mention this here. The key preventative technique for this injury is training the abdominals and the obliques. High reps and preferably on an unstable surface. You can also add BFR (blood flow restriction training) to your core routine and this will not only push your endurance but aid in building strength. I will have athletes do 8-10 sets of 10-15 reps of abdominals and obliques on a physioball to help prevent. If doing BFR, I will have them do 4-6 sets of 30 reps in each direction.

We hope you continue to enjoy this series and find the information valuable. In the next article, we will get into some specific stretches and exercises for preventing injuries. If you did enjoy, please share with your colleagues, training partners and BJJ enthusiast and please be sure to follow us on instagrm @ bjjpt_acl_guy and twitter @acl_prevention. #ViPerformAMI #ACLPlayItSafe
Read more:




