Baseball, Health
Welcome and thanks for visiting...

Elbow and Shoulder Injuries in Youth Athletes During Growth Spurts
The number of children participating in youth sports is growing each year and so is the number of sports related injuries. Research indicates that injuries in children make up approximately 5% of all visits to medical doctors. During adolescence (ages 10 to 19), the number jumps to 10% with more boys than girls affected. Most injuries to young athletes are related to overuse and occur gradually over time, when an athletic activity is repeated so often that the affected areas of the body do not have enough time to heal between activities.
Why the increase. Prior to puberty, sports injuries are not very common. But just before, during and after puberty, there are significant changes in muscles and bones that can increase the risk of injury. With the onset of puberty, bone length grows at a faster rate than muscles and tendons. Bones increase in length; muscles increase in size. Because bone length is increasing at a faster rate than muscle and tendon length, the muscles become tight which, in turn, reduces flexibility. An increase in muscle tightness (lack of flexibility) can also increase the pulling force on the growth plate of bones at the attachment site and can cause pain and inflammation. If the situation is not treated and/or the athlete continues to train and play, does not improve flexibility and does not give the apophysis time to heal, the pain will increase. In the worst cases, the cartilage can be pulled away from the bone resulting in an avulsion fracture.
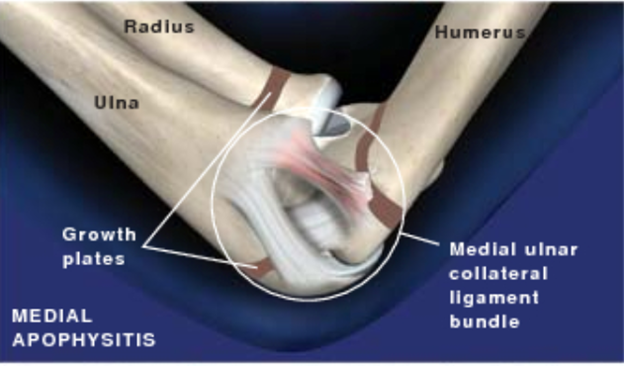
Muscles attach to bones by tendons. In young athletes, the sites of attachment are called apophysis. These sites are growth plates made of cartilage that is weaker than bones and muscles. When a muscle contracts to move a bone, it tugs on the apophysis (growth plate). When these tugs occur repeatedly, with too much force or with bad mechanics, they can, over time, injure the cartilage and cause, inflammation, swelling and pain (apophysitis).
Many sports medicine specialists believe that the increasing number of sports injuries in young athletes is attributed to early specialization and year-round participation in sports. In the past, children changed sports with the seasons. Today it is common for some children to play on more than one team at the same time while others participate in a single sport, all year long. This repetitive use of the same muscle groups places unchanging stress to specific areas of the body, leading to muscle imbalances that, when combined with overtraining and inadequate rest periods, can put young athletes at serious risk for overuse injuries.
What are the signs and symptoms of apophysitis? Common signs and symptoms include:
- Pain, swelling and tenderness over a growth plate where a muscle tendon attaches that often increases with activity, and can’t be tied to an acute injury, such as from a collision or fall
- Pain that typically worsens with activity, improves with rest and sometimes causes a limp
- Changes in running, throwing, jumping form or technique
Who gets apophysitis? Young athletes who are involved in sports that require repetitive action of the same joint or joints are most susceptible, especially those involved in throwing sports like baseball, jumping in basketball and running in track and soccer.
What are the risk factors for apophysitis?
- Active, growing children and adolescents
- Rapid growth
- Lack of flexibility
- Muscle weakness
- Pushing through activity-related pain
How is apophysitis diagnosed? Often, apophysitis is a clinical diagnosis made in a doctor’s office or clinic. The physician will review the patient’s pain history and location of pain when making a preliminary diagnosis. Sometimes X-rays, MRI or CT scan will be recommended to confirm the preliminary diagnosis or rule out an avulsion fracture or other serious conditions.
How is apophysitis treated? Rest and physical therapy are required to completely heal an inflamed growth plate and safe return to sports. Complete recovery of the epophysitis usually takes 4-8 weeks depending on the severity of the injury, but every athlete is different. Physical therapists will focus on improving flexibility, joint stability, movement mechanics and strength in the muscles around the injured area to facilitate healing and minimize the risk of re-injury. Pediatric sports medicine specialists recommend a conservation return to play to help ensure a safe return to sports and minimize the risk of reinjury. Athletes are often allowed to return to play when there is no pain when running, squatting and jumping. If an athlete experiences pain or limping during these activities, additional physical therapy is recommended and return to play is delayed.
The two most common overuse injuries in young baseball players are little league elbow (pain on the bony part of the inner part of the elbow) and little league shoulder (pain in the upper part of the arm at the shoulder). After the bone heals, it doesn’t mean you can immediately return back to games. For every week down not throwing to let the bone to heal, you need the same number of weeks to build up a throwing program prior to returning back to the game without restrictions.
Medial epicondyle apophysitis, often called "little league elbow," is the most common injury affecting young pitchers whose bones have not stopped growing. It is caused by overuse of the muscles of the elbow and forearm. Data suggest that approximately 25% of youth pitchers and 58% of high school pitchers experience medial elbow pain at some point during their playing time. Those affected will have pain on the bony part of the inner elbow (medial epicondyle) caused by irritation and inflammation of the growth plate (apophysis) on the inner side of the elbow. In addition to pain when throwing, players will exhibit point tenderness over the medial epicondyle and a marked decrease in throwing speed and distance. Some also have flexion contracture which limits their ability to fully extend the elbow.
What causes little league elbow? As previously stated, this is an overuse injury caused by throwing too much, too hard and/or too often. Data suggests that there is a direct link between medial elbow pain and the number of pitches and the number of games in which a pitcher throws, especially in those who play year-round and pitch for more than one team.
Most leagues have rules that limit how many pitches a player is allowed to throw in a game, week and tournament. These rules, however, do not take into account the number of throws in pre-game warm-up, pitches between innings or the extra throwing done outside of practice and games. Counting the total number of throws is important because muscles fatigue with excessive throwing. Fatigue is cumulative and is not just caused by throwing too many pitches in a game. It’s also related to throwing too many pitches in an inning, too many pitches in a season and too many pitches in a year.
It’s important to note that mental stress can increase fatigue. The stress on a pitcher who throws 35 pitches in two innings with no one on base is much less than that of a pitcher who throws the same number of pitches with runners in scoring position. Making a note of the number of stressful innings and pitches thrown in stressful innings can prove to be a valuable tool in helping manage fatigue in young pitchers.
The primary stabilizing forces for the elbow are provided by the muscles of the elbow and forearm and ulnar collateral ligament (UCL) on the medial or inside of the elbow joint. When the muscles fatigue, they lose their ability to stabilize the elbow and the UCL is forced to become the primary stabilizer of the inside of the elbow. Overuse of the elbow can cause the UCL to weaken resulting in a sprain and lead to pain in the elbow, popping or shifting in the joint, decreased range of motion in the joint and loss of control and power when pitching. In the early stages of overuse, pitchers might experience a mild sprain of the UCL. If left untreated and subjected to continued stress, the repetitive stress can cause the UCL to rupture and possibly lead to “Tommy John Surgery”.
What are the signs and symptoms of little league elbow? The appearance of any of the following symptoms should be cause for concern:
- Pain or tightness while throwing
- Tightness or loss of range of motion after throwing
- Soreness that lasts for several days after pitching/throwing
- Loss of velocity or control of pitches
- Swelling in the forearm, elbow or shoulder
- Numbness in the forearm or hand, especially in the ring and little fingers
How is little league elbow treated? Anytime a young throwing athlete complains of medial elbow pain, parents and coaches should suspect that it might be little league elbow. Early recognition and intervention are extremely important and can lead to better treatment outcomes and decrease the risk of permanent damage or persistent functional disability. Because these types of injuries are often age dependent, the medical management will ultimately depend on the underlying cause of the symptoms. Treatment usually consists of complete rest from throwing activities for a minimum of 4-6 weeks, ice and non-steroidal anti-inflammatory medication (NSAIDs), physical therapy and a gradual return to a progressive throwing program once the athlete is pain free.
How is the risk of little league elbow reduced? Risk can be reduced when parents and coaches work together to avoid overuse. How do you do this?
- Compare age to hours of participation. One way is to look at age vs. hours of participation. Research on young athletes suggests that young athletes who spend more hours per week than their age playing one sport are 70% more likely to experience overuse injuries than other injuries. A 14-year-old, for example, who plays and practices 15 hours of baseball per week should be at increased risk for an overuse injury. As a general rule of thumb, a young athlete should not be spending more hours per week in a sport or sports than their age. A 14-year-old should spend no more than 14 hours per week playing or practicing his/her sport.
- Schedule rest breaks / time outs. Another effective approach is to schedule rest breaks. Sports medicine specialists recommend that athletes should rest 1-2 days each week and take longer breaks throughout the year to minimize the risk of overuse.
- Maintain free-lines of communication. It’s also important that parents and coaches have a free and open line of communication with team members. Players should feel free to let their parents and coaches know if they are experiencing pain, discomfort or if something just doesn’t feel right. Overuse injuries don’t develop overnight, so it’s important to address them quickly to minimize recovery time and potential long-term effects. It’s easier to prevent a fire than to put it out and rebuild the structure.
- Know your child / players. Parents should know their children best and a good coach should know his/her players. Both should keep close tabs on each player’s performance and behavior so they can quickly recognize if something is off. As Yogi said, “You can see a lot by watching.” Listen when a child tells you something hurts. It’s impossible to play through an overuse injury. Always err on the side of caution.
- Encourage athletes to play multiple sports. The movements in baseball are different than those of soccer and basketball and develop different muscle groups and different types of agility, balance, coordination and body control. Playing multiple sports will help improve athleticism and reduce the physical and mental stress of playing just one sport.
- Understand the science. Baseball USA and prominent sports medicine specialists have concluded that young players, especially pitchers increase the risk of injury if they throw too many innings per year. Research indicates that those who pitch more than 100 innings in a year are 3.5 times more likely to have an injury. Those who play for multiple teams at the same time are also at increased risk as are those who continue to throw despite arm fatigue. Pitchers who throw when fatigued are 36 times more likely to suffer an injury. Other factors that have been shown to contribute to injury are playing more than 8 months per year and frequent participation in showcases.
Some high school associations have adopted guidelines that limit the frequency with which pitchers can throw in games depending on the number of pitches thrown in their last outing. The information in the table below indicates that a pitcher who throws 30 or fewer pitches on Friday can pitch again on Saturday. If, however, he throws 51-75 pitches, he has to rest two full calendar days before he can pitch again, i.e., he can pitch again on Monday. The recommended maximum number of pitches allowed in a single day is 105. A pitcher who throws 105 pitches on Friday, would need at least three days of rest before he could pitch again. He could pitch again on Tuesday.
Pitch counts help control overuse stresses that accumulate over time. Mandating rest periods between games helps ensure that the body has enough recovery between pitching appearances to allow body tissue, especially those in the arm and shoulder to fully recover. This can be extremely important during growth spurts when growth plates are not fully ossified and flexibility is reduced.
|
Day’s rest recommended between appearances for pitchers |
|
|
Number of pitches |
Mandated days rest |
|
1-30 |
0 |
|
31-51 |
1 |
|
51-75 |
2 |
|
75-105 |
3 |
What is little league shoulder? Little league shoulder (proximal humeral apophysitis is an overuse injury to the throwing arm at the shoulder joint. It is caused by stress to the upper arm bone (humerus) growth plate. Excessive stress to this site can stress and irritate the growth plate, resulting in swelling and pain at the shoulder. It is common in pitchers between the ages 11 and 16 and most common among 13- and 14-year-old pitchers who are still growing and transitioning to larger diamonds with longer distances between home plate and pitcher’s mound. Data suggest that approximately 30-40% of youth and high school pitchers experience shoulder pain at some point during their playing time. The good news is that little league shoulder
often heals completely with rest and a dedicated rehabilitation program. If untreated, the condition can worsen and potentially lead to bone damage.
What causes little league shoulder? Like little league elbow. Many of the factors that contribute to it are similar to those associated with little league elbow plus:
- Repeated overhead throwing without proper rest
- Pitching and throwing with improper mechanics
- Lack of muscle strength, specifically in the shoulder and upper back
What are the signs and symptoms of little league shoulder? Little league shoulder is a chronic overuse injury and usually has a gradual onset of a sudden pain. Parents and coaches should be suspicious if there is an appearance of:
- Pain in the shoulder while throwing, especially after an increase in the number of throws or while trying to increase velocity
- Pain or soreness that lasts for several days after pitching / throwing
- Swelling in the shoulder
How Is little league shoulder treated? Once the diagnosis of little league shoulder is made, the doctor will decide the best possible treatment. In most cases, conservative management will be recommended to include:
- Rest and avoid throwing activities for a period of time
- Ice to decrease swelling, bleeding and pain in the shoulder
- Physical therapy to increase strength in the muscles of the arm and shoulder, improve range of motion in the shoulder joint, increase core strength/stability, improve strength in the hips/legs and improve total body control/coordination from the ground up
- Once cleared to return to throwing, the athlete will be given a progressive throwing program that slowly increases the forces and demands through the arm and shoulder needed for full return to competitive play
How is the risk of little league elbow and shoulder reduced? While it is impossible to prevent all injures, research and experience indicates that players who observe the following guidelines tend to have a reduced risk of injury:
- Warm up and stretch before exercise, practice or play
- Gradually cool down after activity
- Perform daily arm care exercises to strengthen the muscles of the shoulder blade, rotator cuff, core, low back, hip and legs
- Ice stiff or sore joints after exercise
- Stop throwing and seek help with soreness or pain
- Because of the volume of throwing required, the risk of arm and shoulder injury is greater in those that both catch and pitch
Conclusion. Adolescent athletes are injured most often during or just after periods of rapid growth. Most injuries are due to overuse caused by the extreme stress that repetitive throwing can place on immature bones and developing soft tissues. The combination of repetitive throwing, weak cartilage at growth centers, muscle tightness associated with rapid long bone growth, increased laxity of soft tissue, and inefficient movement patterns can often place an adolescent athlete at increased risk of elbow and shoulder injury.
Parents and coaches should be aware of the risk factors associated with overuse injuries and strive to stay within the guidelines established by sports medicine specialists to help ensure safe participation of all youth athletes, especially those in sports that require repetitive overhead throwing.




